44 yr old male patient complaints of pedal edema since 10 days and decreased urine output since 5 days
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
Chief complaints:
A 44year man who is a farmer by occupation came to OPD with chief complaints of:
1)B/L pitting type of pedal edema since 10 days and decreased urine output since 5 days
2)pain in the abdomen since 4 days
3)vomiting since a day.
History of presenting illness:
He was apparently asymptomatic 1 and 1/2 yrs back , then he developed swelling in face and lower limbs and visited doctor , and was on medication . He stopped medication after 10 days.
After few days he had difficulty in breathing (SOB grade 2) and decreased urine output
He was admitted to hospital and was on dialysis for 2 days .
Since then he was on dialysis twice every week.
Patient was apparently asymptomatic 10 days back and gradually developed B/L pitting type of pedal edema which was & decreased urine output.
Patient developed pain in the epigastric region since 4 days ,which is of pricking type, non radiating, aggravated after food and relieved on its own after some time .
Patient also showed history of vomiting of 6-7 episodes which was non bilious , consisted of food particles and was relieved on medication .
Past history:
K/C/O HTN since 4 years, but he didn't take any medication for it.
N/K/C /O DM ,TB , EPILEPSY, ASTHMA.
Personal history:
Diet: mixed
Appetite: normal
Sleep: adequate
Bowel n bladder: irregular , decreased urine output progressed to anuria.
Addiction: alcohol consumption qty: 180ml 3-4 times a week at night , since 15years, stopped since 1and 1/2 year.
No History of smoking
Family history:




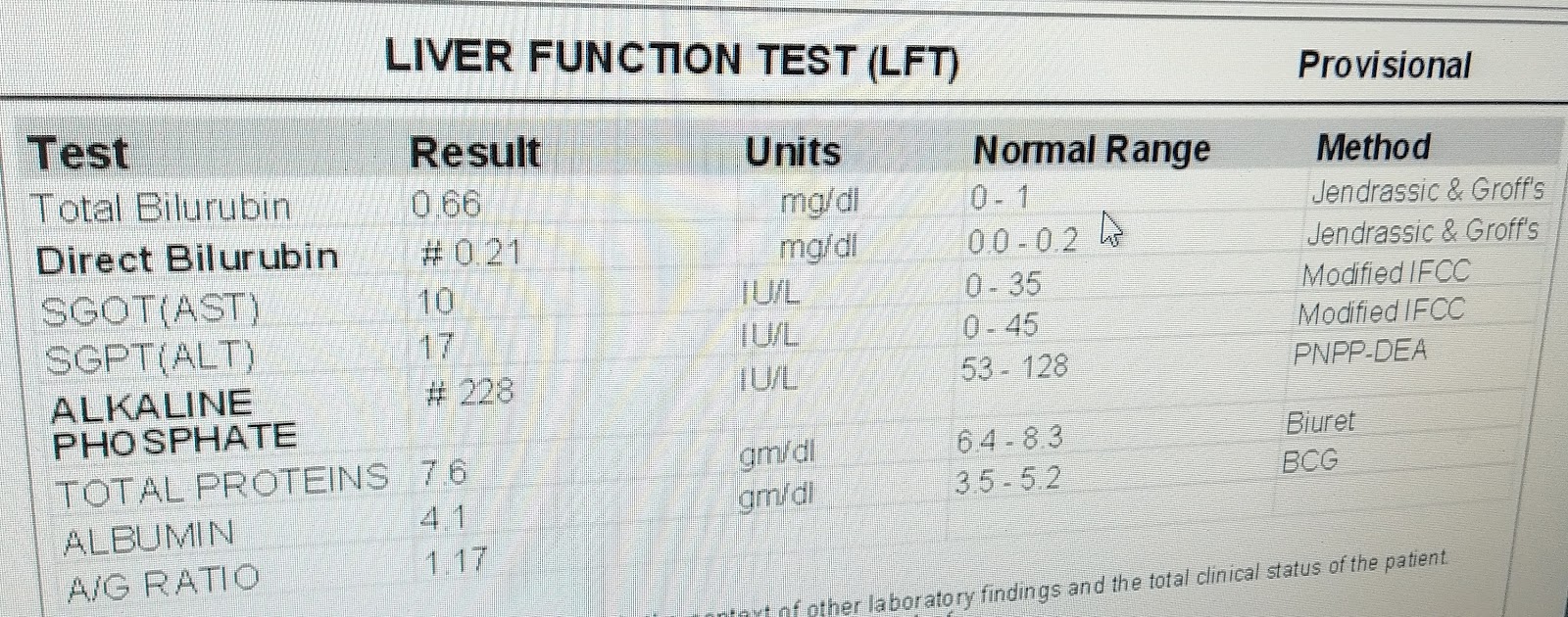
LFT:

ABG:


HEMOGRAM:

ABG



Plan of treatment:
1.Fluid and salt restriction
2. INJ. ZOFER 4 mg IV/ TID
3. INJ. TRAMADOL 1 AMP in 100 ml NS IV / SOS
4. TAB. NICARDIA 10 mg PO/TID
5. TAB. ARKAMIN 0.1mg PO/BD
6. TAB. MET- XL 25 mg PO/OD
7. TAB. SHELCAL 500mg PO/ OD
8. Cap. BIO-D3 PO/OD/WEEKLY ONCE
9. INJ. ERYTHROPOIETIN 4000 IU S/L WEEKLY TWICE
10. BP MONITORING 2nd hrly
11. GRBS 2nd hrly.
Chief complaints:
A 44year man who is a farmer by occupation came to OPD with chief complaints of:
1)B/L pitting type of pedal edema since 10 days and decreased urine output since 5 days
2)pain in the abdomen since 4 days
3)vomiting since a day.
History of presenting illness:
He was apparently asymptomatic 1 and 1/2 yrs back , then he developed swelling in face and lower limbs and visited doctor , and was on medication . He stopped medication after 10 days.
After few days he had difficulty in breathing (SOB grade 2) and decreased urine output
He was admitted to hospital and was on dialysis for 2 days .
Since then he was on dialysis twice every week.
Patient was apparently asymptomatic 10 days back and gradually developed B/L pitting type of pedal edema which was & decreased urine output.
Patient developed pain in the epigastric region since 4 days ,which is of pricking type, non radiating, aggravated after food and relieved on its own after some time .
Patient also showed history of vomiting of 6-7 episodes which was non bilious , consisted of food particles and was relieved on medication .
Past history:
K/C/O HTN since 4 years, but he didn't take any medication for it.
N/K/C /O DM ,TB , EPILEPSY, ASTHMA.
Personal history:
Diet: mixed
Appetite: normal
Sleep: adequate
Bowel n bladder: irregular , decreased urine output progressed to anuria.
Addiction: alcohol consumption qty: 180ml 3-4 times a week at night , since 15years, stopped since 1and 1/2 year.
No History of smoking
Family history:
There is no significant history seen in the family.
General examination:
Patient is conscious, coherent and cooperative and well oriented to time, place and person,
On examination:
General examination:
Patient is conscious, coherent and cooperative and well oriented to time, place and person,
On examination:
VITALS:
Pallor present( mild) , no icterus/ clubbing/ cyanosis / lymphadenopathy /edema (apparently)
Temp: 98°F
BP : 140/100mmHg
RR: 28/min
PR : 80/min
SPO2: 99% @ RA
Temp: 98°F
BP : 140/100mmHg
RR: 28/min
PR : 80/min
SPO2: 99% @ RA
SYSTEMIC EXAMINATION :
CVS: S1 S2 +
RS : BAE +
CNS : NAD
P/A : tenderness and pain in the epigastric region
CVS: S1 S2 +
RS : BAE +
CNS : NAD
P/A : tenderness and pain in the epigastric region



Investigations:
RFT:
RFT:

LFT:
ABG:

ECG:

HEMOGRAM:

ABG

SERUM ELECTROLYTES:

TROPONIN:

Provisional diagnosis:
?acute gastritis
CKD on MHD, HTN +
CKD on MHD, HTN +
Plan of treatment:
1.Fluid and salt restriction
2. INJ. ZOFER 4 mg IV/ TID
3. INJ. TRAMADOL 1 AMP in 100 ml NS IV / SOS
4. TAB. NICARDIA 10 mg PO/TID
5. TAB. ARKAMIN 0.1mg PO/BD
6. TAB. MET- XL 25 mg PO/OD
7. TAB. SHELCAL 500mg PO/ OD
8. Cap. BIO-D3 PO/OD/WEEKLY ONCE
9. INJ. ERYTHROPOIETIN 4000 IU S/L WEEKLY TWICE
10. BP MONITORING 2nd hrly
11. GRBS 2nd hrly.


Comments
Post a Comment